What are they?The menisci are elastic structures sitting between the femur (thigh bone) and tibia (leg bone) inside the knee joint. There are two menisci (medial & lateral) in each knee. They act as wedge shaped shock absorbers between the bones. Each wedge shaped meniscus is curled to form the shape of the letter C between the thigh & leg bone. Each meniscus is anchored peripherally (on its outer aspect) to the lining of the knee joint (capsule).
Injuries to the menisci are often referred to as "cartilage" injuries leading to a possibility of confusion. When referring to a cartilage injury one has to distinguish between the true "articular" cartilage ie the joint surface of the knee or the meniscal cartilage injury ie the injury specific to the meniscus itself. Meniscal injuries consist of a variety of tears. These tears may occur either as a small tear of the free edge (called parrots beak tear), a split in the horizontal plain (cleavage tear) or a detachment around the peripheral attachment (bucket handle tears).
How does a meniscus tear?
In younger people, this usually happens after a twisting injury at sport of even during regular daily tasks. A meniscal tear is more likely to happen if you have a previous ligament injury to your knee such as a ruptured anterior cruciate ligament. A meniscal tear may happen without a significant injury in older people who have some wear & tear (early arthritis) changes in the knee (degenerative tear).
 What does a meniscal tear feel like?
What does a meniscal tear feel like?
A meniscal tear causes pain and discomfort in the region of the joint line ( ie the point of attachment of the meniscus to the lining of the knee). Occasionally, the torn fragment of the meniscus displaces within the knee joint and is trapped between the thigh & leg bones causing clicking & even locking of the knee. A locked knee is a knee that will not straigten fully but does bend. This condition should be treated with a degree of urgency to prevent any further damage to the meniscus which if maintained in reasonable condition may be repairable.
How can I tell if my meniscus is torn?
Your doctor will examine you and most of the time will organise for you to have an MRI scan to confirm the diagnosis.
What should be done about my meniscal tear?
Unfortunately, If a meniscal tear is causing significant pain, the only possible treatment is surgery. This consists of an arthroscopy (key hole operation) of the joint to treat the tear. If the knee is locked, the arthroscopy may be proceeded with with a degree of urgency.
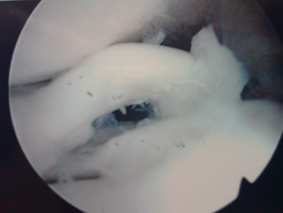
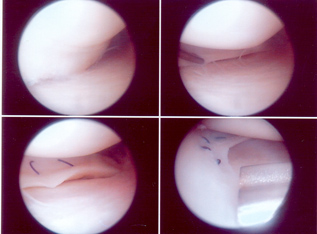 What happens at surgery?
What happens at surgery?
If the fragment of torn meniscal cartilage is not repairable it is best removed and the damaged tissue trimmed back to healthy stable tissue. As little as possible is removed of the meniscus. This operation generally can be done as a day case operation (though occasionally an overnight stay is required). The operation is done through two or three small incisions through which the damaged tissue may be removed. Recovery is normally swift and within two weeks the stitches can be removed and practically full activity achieved. Driving is normally restricted until an emergency stop can be safely performed - the time to achieve this is variable and may be as short as a few days or as slow as two weeks. Return to work may be achieved rapidly if office based but may take a number of weeks if returning to a physical job.
.jpg)
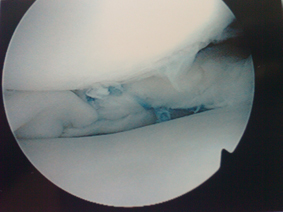
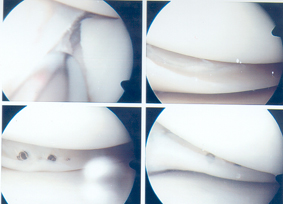
If the fragment of torn meniscus is repairable (this normally occurs when the tear in the tisuue is close to the peripheral edge of the meniscus where it is attached to the joint capsule - frequently this is a bucket handle tear). Repair involves stitching the meniscus and then protecting the repair by keeping you non-weight bearing or putting minimal weight through the joint using crutches for support. Stitches may be placed from outside the joint into the joint or placed within the joint and brought out to the skin. Occasionally there may be a type of dissolvable stitch used entirely inside the joint. All these methods indicated above are performed using key hole methods and will normally end up with some minor skin scars around the area of the repair. If the meniscus is repaired then the progress is much slower than if the torn fragment is excised but in the long term it may be better to try to save the meniscus as its function is important in preventing the onset of arthritis.
Back to top